

One Traumatized Medicaid Patient, Eight Fake Phone Numbers, and an Algorithm Waiting to Cut Her Off. This Is Where Your Tax Dollars Go.
High mental illness rates in Medicaid + fraud + UnitedHealth algorithms = taxpayer money down the drain instead of actual care.

A licensed therapist wanted to treat one traumatized young woman on Medicaid.
He spent an entire morning on the phone with eight different organizations. Fake phone numbers. Bounced emails. Placeholder help desks that spit out 111-111-1111. Reps who couldn’t even get him logged in to see the patient.
This wasn’t a glitch. This is the Medicaid mental health “network” working exactly as designed.
And here’s the part that should make every taxpayer furious: even if that therapist had somehow fought through the ghost network and started seeing her, UnitedHealth was already queued up with its next move.
According to a ProPublica investigation, UnitedHealth (through Optum) rolled out internal algorithms specifically targeting outpatient mental health care in its Medicaid plans. The system flagged patients for “overutilization” — things like more than 30 therapy sessions in eight months or twice-a-week visits. The same company that settled with California, New York, and Massachusetts regulators for illegally applying stricter rules to mental health than to physical health kept running these reviews anyway. They did it in Medicaid plans serving the poorest and most vulnerable patients in roughly two dozen states.
Taxpayers are footing the bill for these plans. Government money is supposed to treat people in the middle of a real mental health crisis. Instead, we get a two-layered scam:
Contractors who build fake networks so providers can’t even get in the door.
Insurers who let providers in… then override doctors to cut off the care.
This isn’t “managing costs.” This is laundering taxpayer dollars through phantom networks and phantom care while real patients get nothing.
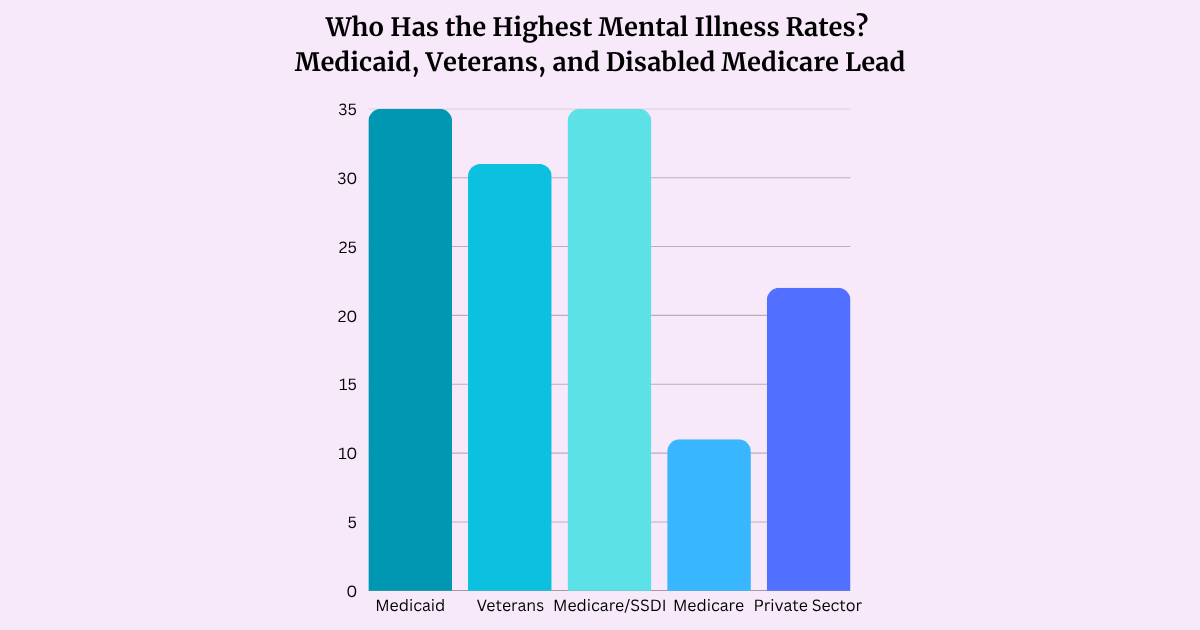
Medicaid serves the populations with the highest mental health needs — not luxury cases. Here’s how prevalence compares across major groups (primarily nonelderly adults where data allows direct comparison, sourced from KFF/NSDUH and VA reports):
Medicaid (non-elderly adults): 35% any mental illness, 10% serious mental illness
Veterans (using VA care): ~31% with a confirmed mental health diagnosis; PTSD rates 15–23% (much higher among combat veterans)
Medicare (disabled/SSDI-eligible, non-elderly): Rates often approach or overlap with Medicaid levels due to disability; overall Medicare (mostly 65+) is lower at ~11% any mental illness for seniors
Private insurance (non-elderly adults): ~20–25% any mental illness, ~4–6% serious mental illness
These numbers explain why the system’s barriers hit hardest here. Medicaid (and overlapping veteran/disabled populations) covers the exact groups taxpayers fund to support — trauma, poverty, service-related conditions, and serious impairment — yet the barriers block both entry and continuation of care.
Enough. Here’s what actual policy fixes look like. Not slogans, not “just stop it,” but concrete changes that would force real care:
Verifiable networks or no contract. Mandate real-time, audited provider directories. If fewer than 80% of listed mental health providers are actually reachable, accepting new patients, and properly credentialed, the managed-care organization loses the Medicaid contract in that region and pays daily fines until fixed. No more ghost networks.
One working enrollment portal. Kill the eight-contractor runaround. Require a single, functional, state- or federally-run credentialing system for Medicaid mental health providers. If a licensed therapist wants to treat a patient, they should be able to log in and start in days — not weeks of dead-end calls.
True parity enforcement with teeth. Mental health reviews must use the exact same medical-necessity standards and algorithms applied to physical health conditions. No special “outlier management” programs that only target therapy. Violations trigger automatic repayment of denied claims plus treble damages to the state.
Payment tied to actual treatment delivered. Stop the per-member-per-month gravy train that rewards insurers for enrolling people they never intend to treat. Shift a meaningful chunk of payment to fee-for-service for delivered care, with public dashboards showing utilization rates, denial rates, and network adequacy scores. Make the data impossible to hide.
Claw back the waste and phantom payments. Independent third-party audits of networks and “phantom enrollees.” Any dollars paid for care that never happened get recovered — with interest — and go straight back into expanding real provider capacity.
Pro-Tip: Become the CEO of Your Own Healthcare — What You Can Do Right Now as a Medicaid Patient
You can’t fix the whole system today, but you can stop being a passive passenger. Here’s how to push back on ghost networks, therapy cut-offs, and insurer overrides:
Verify providers yourself — Never trust the online directory alone. Call (or have a friend/family call) every listed therapist before your appointment. Ask: “Do you currently accept new Medicaid patients from [your specific plan]?” Document the date, time, and name of the person you spoke with. If it’s a dead end, report it immediately to your state Medicaid agency as this creates a paper trail that regulators actually use.
Document everything — Keep a simple log of every call, email, denial letter, and conversation. Note dates, names, and what was said. When a session limit or “over-utilization” flag hits, ask your therapist to write a detailed letter explaining medical necessity and comparing it to how physical health conditions (like physical therapy) are handled. This strengthens appeals.
Appeal denials aggressively — You have the right to appeal under federal mental health parity laws. File quickly (deadlines are short). Use the denial reason to argue it treats mental health worse than medical/surgical care. Many appeals succeed on the second or third round, especially with provider support. Contact your state Medicaid ombudsman or consumer advocate office for free help navigating this.
Escalate when needed — If the plan stonewalls you, file a complaint with your state Medicaid agency (find it via medicaiddirectors.org). For parity violations, also report to the federal Parity Complaint Registry or your state insurance department. Persistence + documentation often forces movement.
Explore every door — Ask about telehealth options, community mental health centers, or sliding-scale providers while you fight the system. If you’re a veteran or dually eligible, check VA or other overlapping benefits.
You are the CEO of your care. The system is designed to wear you down. Don’t let it. Document, verify, appeal, and escalate. Every paper trail you build helps expose the BS and pressures change.
The mental health crisis isn’t abstract. The people stuck in Medicaid — and overlapping high-need groups like veterans and disabled Medicare beneficiaries — are often the ones hit hardest by trauma, poverty, service-related conditions, and lack of access. They don’t need more studies, more reports, or more settlements that change nothing. They need a system that actually connects a therapist to a patient and then gets out of the way so treatment can happen.
Right now, UnitedHealth and the rest of the managed-care middlemen are collecting billions in taxpayer money while building barriers on both sides of the exam room. That’s not oversight. That’s something we should no longer be tolerating.
It’s time we stop paying for the barriers and start demanding the care.